
Acute diverticulitis is a painful digestive condition that can interrupt daily life fast. One day you may feel generally fine, and the next you may be dealing with sharp lower abdominal pain, fever, nausea, bloating, or a sudden change in bowel habits that makes it hard to work, eat, sleep, or even walk comfortably.
The condition happens when small pouches in the wall of the colon become inflamed. In some people, the problem stays mild and improves with rest, careful diet changes, and medical guidance. In others, it can become serious and lead to complications that need hospital care.
That difference is exactly why this topic matters in real life. Many people have heard of diverticulosis, but not everyone understands when it turns into diverticulitis, what warning signs should never be ignored, or what recovery actually looks like after an acute episode.
This guide explains what acute diverticulitis is, how it feels, what causes it, how doctors diagnose it, what treatment often involves, and what practical steps may help reduce the risk of future attacks. It is designed for education, not self-diagnosis. Severe abdominal pain, fever, vomiting, weakness, or symptoms that suddenly worsen should be assessed by a qualified healthcare professional promptly.
Table Of Contents
- Understanding Acute Diverticulitis
- Types Of Acute Diverticulitis
- Causes Of Acute Diverticulitis
- Symptoms Of Acute Diverticulitis
- Risk Factors
- Diagnosis Process
- Living With Acute Diverticulitis
- Prevention Strategies
- Practical Examples
- Conclusion
- Frequently Asked Questions
- Final Editorial Disclaimer
- References
Understanding Acute Diverticulitis
To understand acute diverticulitis, it helps to start with the colon. The colon, also called the large intestine, is the last major part of the digestive tract. Its job includes absorbing water, processing waste, and moving stool toward the rectum.
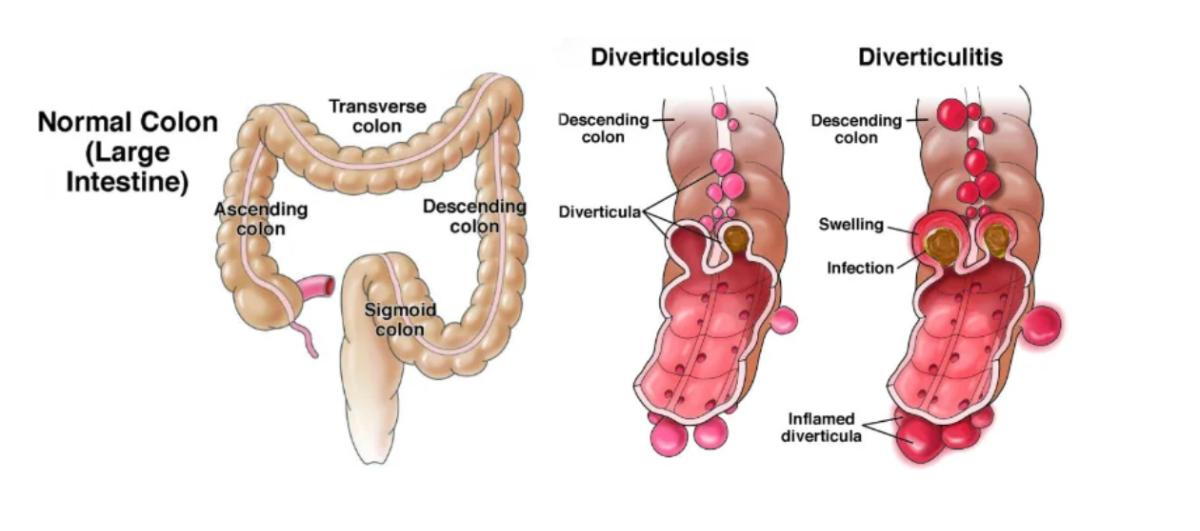
Over time, small bulging pouches can form in weak areas of the colon wall. These pouches are called diverticula. Having these pouches is called diverticulosis. Diverticulosis is common, especially as people get older, and many people never know they have it because it often causes no symptoms.
Acute diverticulitis is different. It means one or more of those pouches becomes inflamed, and sometimes infected. When that happens, the body reacts like it does to other forms of inflammation: pain increases, digestion can feel off, appetite may drop, and the immune system may trigger fever or fatigue.
In everyday terms, think of diverticulosis as “pouches are present,” while acute diverticulitis means “one of those pouches is now causing trouble.”
This distinction matters because the treatment approach changes. A person with incidental diverticulosis found on a screening exam usually does not need urgent care. A person with acute diverticulitis may need anything from home management and close follow-up to IV antibiotics, drainage of an abscess, or surgery if complications develop.
Most cases involve the lower part of the colon. That is why pain often shows up in the lower left side of the abdomen. Still, symptoms can vary, and not every person reads like a textbook.
A practical example helps. Someone may have had occasional constipation or bloating for years and never realize diverticula are present. Then one morning they develop steady lower abdominal pain, feel feverish, lose their appetite, and find that riding in a car or walking upright makes the pain worse. That shift from vague digestive discomfort to a more intense, focused illness is often what leads people to seek care.
Types Of Acute Diverticulitis
Acute diverticulitis is often discussed in two main categories: uncomplicated and complicated.
Uncomplicated Acute Diverticulitis
This is the more straightforward form. There is inflammation, but no major complication such as an abscess, fistula, obstruction, or free perforation.
Symptoms can still feel significant. A person may have:
- Steady lower abdominal pain
- Tenderness when the belly is pressed
- Mild fever
- Nausea
- Constipation or diarrhea
- Bloating
- Reduced appetite
Even though it is called uncomplicated, it should not be dismissed. It still needs proper assessment because other conditions can mimic it, and the treatment plan depends on severity, medical history, and how well the person can drink fluids and function at home.
Complicated Acute Diverticulitis
This form means the inflammation has led to a more serious structural problem. Complications may include:
- Abscess, which is a pocket of infection
- Perforation, meaning a tear or hole in the colon wall
- Peritonitis, a dangerous infection in the abdominal cavity
- Fistula, an abnormal connection between the colon and another organ such as the bladder
- Bowel obstruction or narrowing from swelling or scarring
- Significant bleeding in some cases
Complicated diverticulitis is much more likely to require hospitalization and sometimes procedures or surgery.
First Episode Vs. Recurrent Episodes
Doctors also think about whether the attack is a first episode or one of several. A first episode may feel frightening because everything is new. Recurrent episodes raise different questions, such as whether the diagnosis is certain, whether the colon has healed fully, and whether longer-term prevention or surgical planning should be discussed.
Mild Vs. Severe Clinical Presentation
Another useful way to think about acute diverticulitis is how sick the person actually feels.
A mild presentation may involve pain, tenderness, and a low fever, but the person can still drink fluids, rest, and follow instructions at home.
A more severe presentation may include:
- High fever
- Worsening pain
- Vomiting
- Inability to keep fluids down
- Significant weakness
- A rigid or very tender abdomen
- Signs of infection or dehydration
That is why two people with the same diagnosis may have very different treatment plans.
Causes Of Acute Diverticulitis
The exact trigger is not always obvious in one individual case. In simple terms, acute diverticulitis develops when a diverticulum becomes inflamed. Infection may be involved, but inflammation itself is central to the problem.
Several factors may contribute.
Pressure And Weak Spots In The Colon Wall
Diverticula are thought to form where pressure builds inside the colon over time and pushes the inner lining outward through weaker areas. That does not automatically cause diverticulitis, but it creates the setting in which diverticulitis can happen later.
Blockage Or Irritation In A Diverticulum
One theory is that stool or debris may become trapped in a pouch, leading to irritation, bacterial overgrowth, or reduced blood flow in that area. The pouch then becomes inflamed.
This helps explain why symptoms can begin suddenly. A person may have had diverticula for years without issue, then a specific pouch becomes irritated enough to trigger an acute attack.
Changes In The Gut Environment
The colon is full of bacteria, and the balance of the gut environment matters. Inflammation, shifts in the microbiome, stool patterns, and local tissue stress may all play a role.
That does not mean acute diverticulitis is caused by one single food or one bad meal. In most cases, it is more complex than that.
Chronic Constipation And Straining
Constipation and repeated straining may increase pressure inside the colon. This pressure may contribute to diverticular disease over time and may make flare-ups more likely in some people.
Low-Fiber Eating Patterns Over Time
A low-fiber diet is often discussed because fiber helps stool stay softer and move more efficiently through the colon. Lower fiber intake may be associated with less ideal stool movement and more pressure inside the bowel.
This is one reason healthcare professionals often focus on fiber after the acute phase has settled, not during the height of severe symptoms.
Inflammation Rather Than A Simple Infection Story
Many people assume diverticulitis is always just an infection in the colon. That is too simplistic. Some cases do involve infection, and antibiotics may be needed in selected situations. But current medical thinking recognizes that not every mild case behaves the same way, and inflammation is a major part of the process.
That is important because people sometimes expect a one-size-fits-all treatment. In real practice, treatment depends on the severity of symptoms, imaging results, immune status, complications, and overall risk.
Symptoms Of Acute Diverticulitis
The most common symptom is abdominal pain, usually on the lower left side. This pain is often steady rather than crampy, and it may build over hours or a day.
Many people describe it in very practical ways:
- “It hurts when I stand up straight.”
- “The pain is in one spot and won’t go away.”
- “I don’t feel like eating.”
- “My belly feels sore when the car hits bumps.”
- “I thought it was constipation, but it got worse.”
Common Symptoms
Symptoms may include:
- Lower left abdominal pain
- Abdominal tenderness
- Fever
- Chills
- Nausea
- Vomiting
- Constipation
- Diarrhea
- Bloating
- Loss of appetite
- Feeling tired or generally unwell
Not everyone has every symptom. Some people have strong pain with very little fever. Others feel feverish and weak before the pain becomes intense.
Symptoms That May Suggest A More Serious Problem
These signs deserve urgent medical attention:
- Severe or rapidly worsening abdominal pain
- Inability to keep liquids down
- High fever
- Fainting, confusion, or marked weakness
- A swollen, hard, or rigid belly
- Pain with guarding, where the abdomen becomes difficult to touch
- Signs of dehydration
- Blood in the stool
- Trouble urinating, or air in urine, which may suggest a fistula in some cases
Symptoms In Daily Life
Acute diverticulitis often affects routine activities more than people expect. Sitting at a desk may become uncomfortable. Bending, lifting groceries, walking quickly, and eating a full meal may all feel worse.
Some people initially mistake it for gas, food poisoning, or a stomach bug. The difference is often the persistence and location of the pain. Gas pain usually shifts. Acute diverticulitis pain often stays in one area and remains tender.

Symptoms After The Acute Phase
Even after a flare improves, some people still notice:
- Temporary fatigue
- Mild bowel irregularity
- Fear of eating normally again
- Anxiety about recurrence
- Occasional abdominal sensitivity
This does not always mean the inflammation is still active, but lingering symptoms should be reviewed if they continue, worsen, or interfere with normal recovery.
Risk Factors
Acute diverticulitis does not happen randomly. Some factors may increase risk or make episodes more likely.
Age
The likelihood of diverticular disease increases with age. Not every older adult develops diverticulitis, but age remains an important risk factor because diverticula become more common over time.
Obesity And Excess Weight
Higher body weight, especially central abdominal weight, is associated with a higher risk of diverticulitis and may also be linked to more severe disease in some people.
Low Physical Activity
A sedentary lifestyle may increase risk. Regular movement supports bowel function, overall metabolic health, and digestive rhythm.
Low-Fiber Eating Pattern
A long-term pattern low in fiber may contribute to less efficient stool movement and more pressure in the colon.
Smoking
Smoking is associated with a higher risk of complications in many digestive conditions, and it may also increase diverticulitis risk.
Certain Medication Patterns
Some medications may be associated with a greater risk of diverticular complications in certain people. These can include nonsteroidal anti-inflammatory drugs, steroids, and some other medicines depending on the situation.
This does not mean people should stop prescribed medications on their own. It means medication history matters and should be reviewed with a clinician.
Immune Suppression
People with weakened immune systems may be at higher risk for complications and may need a lower threshold for medical evaluation and treatment.
Past History Of Diverticulitis
Once someone has had an episode, recurrence becomes part of the conversation. Some people never have another attack. Others may have repeated episodes over time.
Diet Quality And Overall Lifestyle
A broader healthy eating pattern appears to matter more than obsessing over one specific “forbidden” food. Many people still believe nuts, seeds, and popcorn must always be avoided. That older idea has not held up well. In most cases, the larger pattern of fiber intake, hydration, physical activity, weight management, and smoking status matters more.
Diagnosis Process
Acute diverticulitis is not something people should diagnose on symptoms alone. Many abdominal conditions can overlap, including appendicitis, kidney stones, urinary infection, inflammatory bowel disease, irritable bowel syndrome, ovarian problems, and colon-related conditions.
Medical History
A clinician usually starts by asking:
- Where is the pain?
- When did it start?
- Is it constant or comes in waves?
- Any fever, chills, nausea, or vomiting?
- Any constipation or diarrhea?
- Any previous episodes?
- Any recent colonoscopy?
- Any medication use, especially pain relievers or steroids?
- Any history of bowel disease, surgery, or immune suppression?
These questions help sort out how urgent the situation may be and what else needs to be ruled out.
Physical Exam
The abdomen is checked for tenderness, bloating, guarding, and signs that the lining of the abdomen may be irritated. A very tender, rigid abdomen raises concern for complications.
Blood Tests
Blood work may be used to look for signs of infection, inflammation, dehydration, or other problems.
CT Scan
A CT scan is commonly used when doctors need to confirm the diagnosis or assess severity. It can help show:
- Inflamed diverticula
- Thickening of the colon wall
- Nearby inflammation
- Abscess
- Perforation
- Obstruction
This is one reason CT imaging is so important in moderate to severe cases. It helps distinguish uncomplicated from complicated disease.
Stool Tests Or Urine Tests
These may be used when symptoms overlap with infection, kidney stones, urinary symptoms, or diarrhea-related illness.
Colonoscopy Timing
Colonoscopy is usually not performed during an active acute attack because the colon is inflamed and more vulnerable. After recovery, a clinician may recommend colonoscopy based on the severity of the episode, your age, past screening history, and whether another condition needs to be ruled out.
That follow-up matters because abdominal pain and colon inflammation are not unique to diverticulitis.
Living With Acute Diverticulitis
Living with acute diverticulitis is not just about treating one flare. It is also about understanding recovery, rebuilding confidence around food, and knowing how to manage the uncertainty that can follow.
The Acute Phase
During an active flare, daily life often narrows quickly. People may need to cancel plans, rest more, stay close to a bathroom, or avoid full meals for a short time under medical guidance.
A typical real-life experience may look like this:
- Day 1: Persistent lower abdominal pain and reduced appetite
- Day 2: Tenderness worsens, mild fever starts, eating feels unpleasant
- Day 3: Medical evaluation confirms diverticulitis
- Next few days: Rest, hydration, treatment plan, lighter diet if advised, close monitoring
The main priorities are symptom control, preventing dehydration, and identifying whether complications are present.
Eating During Recovery
Food is one of the biggest sources of confusion.
During an acute flare, some people are advised to follow a clear liquid or low-fiber approach for a short period so the bowel can rest. This is not usually a forever diet. It is a temporary recovery tool.
Once symptoms improve, foods are often reintroduced gradually. Eventually, many people are encouraged to return to a higher-fiber pattern for long-term colon health, depending on the individual situation.
A practical recovery sequence may look like this:
- Clear liquids for a short period if advised
- Low-fiber, easy-to-digest foods as pain settles
- Slow return to regular meals
- Gradual increase in fiber after recovery
Examples of gentle foods during a temporary low-fiber phase may include:
- Broth
- Plain rice
- Toast
- Applesauce
- Yogurt if tolerated
- Eggs
- Mashed potatoes
- Tender chicken
- Pasta
- Well-cooked vegetables without skins in some cases
After recovery, higher-fiber foods may be built back in slowly:
- Oatmeal
- Beans
- Lentils
- Berries
- Pears
- Vegetables
- Whole grains
- Chia seeds
- Bran cereals if tolerated
The keyword is gradually. Pushing too much fiber too fast may lead to bloating and discomfort.
Hydration Matters
Many people focus on fiber and forget fluids. Fiber works best when fluid intake is adequate. Dehydration can worsen constipation and make digestion feel harder.
Activity During Recovery
During the acute stage, rest is often important. After improvement, gentle walking may support recovery and bowel movement. Heavy lifting and intense exercise may need to wait until the person feels better and has medical clearance if the episode was severe.
Emotional Impact
Digestive illnesses can be surprisingly stressful. Some people become afraid to eat certain foods. Others worry every abdominal twinge means another attack.
This anxiety is understandable, especially after a painful first episode. Helpful next steps include:
- Keeping follow-up appointments
- Asking what symptoms are expected during recovery
- Knowing which warning signs are urgent
- Reintroducing foods slowly rather than avoiding everything
- Seeking support if health anxiety starts affecting daily life
Prevention Strategies
Prevention is not a perfect guarantee, but several habits may help lower risk or support long-term colon health.
Build A High-Fiber Eating Pattern After Recovery
For many people, this is one of the most practical long-term strategies. The goal is not to jump from very low fiber to very high fiber overnight. The goal is to steadily improve the overall pattern.
Simple ways to do that:
- Add fruit to breakfast
- Include vegetables at lunch and dinner
- Swap refined grains for whole grains when tolerated
- Use beans or lentils a few times a week
- Increase fiber step by step
Drink Enough Fluids
Water helps stool move more smoothly through the digestive tract. People increasing fiber usually need to pay closer attention to hydration.
Exercise Regularly
Movement supports bowel health, weight management, and overall metabolic health. This does not have to mean intense workouts. Walking, cycling, swimming, and structured exercise can all help.
Maintain A Healthy Weight
Weight management may reduce the risk of future episodes and benefits many other areas of health as well.
Avoid Smoking
Smoking affects tissue health and inflammation in multiple body systems. Quitting may support digestive health in addition to heart and lung health.
Avoid Constipation When Possible
This does not mean using laxatives casually without guidance. It means paying attention to bowel patterns early through:
- Fiber
- Hydration
- Activity
- Routine meals
- Timely bathroom habits instead of ignoring the urge
Review Medication Risks
If you use pain relievers often, especially anti-inflammatory medicines, it may be worth discussing safer options with a healthcare professional depending on your health history.
Do Not Obsess Over One “Bad” Food
Many people want a single culprit. In most cases, it is more useful to focus on overall pattern, tolerance, and consistency than to fear one handful of nuts or one serving of popcorn. Individual tolerance can vary, but strict old food myths do not fit everyone.
Practical Examples
A Simple Recovery Checklist After An Acute Episode
- Follow the treatment plan exactly as prescribed
- Keep up with fluids unless told otherwise
- Use the recommended eating plan for the current stage of recovery
- Rest, but add gentle walking when able
- Monitor temperature and symptom changes
- Seek care promptly if pain worsens, fever persists, or vomiting develops
- Ask when to transition back to normal meals
- Ask whether follow-up imaging or colonoscopy is needed
Sample Beginner-Friendly Meal Progression
This is only a general example. Personal guidance may differ.
Early Recovery Phase
- Water, broth, electrolyte fluids if needed
- Plain gelatin or ice pops if tolerated
- Tea without heavy additives
Transition Phase
- White rice
- Toast
- Scrambled eggs
- Applesauce
- Plain pasta
- Yogurt
- Chicken soup
- Mashed potatoes
Long-Term Maintenance Phase
- Oatmeal with berries
- Lentil soup
- Whole-grain toast
- Brown rice with vegetables
- Beans with cooked vegetables
- Fruit and nuts if tolerated
- Salad added gradually, not all at once if you are sensitive
Daily Routine Example For Prevention
Morning
- Drink water after waking
- Eat a fiber-containing breakfast such as oatmeal with fruit
- Take a short walk if possible
Midday
- Choose a lunch with vegetables and a whole grain
- Avoid skipping meals if that leads to constipation later
Afternoon
- Continue fluids
- Stand up, stretch, or walk if you sit for long periods
Evening
- Eat a balanced dinner with vegetables, lean protein, and fiber
- Avoid going several days without a bowel movement before taking it seriously
- Wind down and get adequate sleep
Do And Don’t List
Do
- Take new or worsening abdominal pain seriously
- Stay hydrated
- Increase fiber gradually after recovery
- Keep follow-up visits
- Ask questions about recurrence prevention
- Pay attention to fever, vomiting, and worsening pain
Don’t
- Assume all abdominal pain is “just gas”
- Start or stop medications casually without medical advice
- Force a high-fiber diet during a severe flare if you were told to rest the bowel
- Ignore persistent fever
- Stay home with severe pain, dehydration, or a rigid abdomen
- Rely only on internet food lists without professional guidance
Common Mistakes People Make
Waiting Too Long To Seek Care
Some people keep hoping the pain will pass. Mild digestive upset may pass. Persistent, localized abdominal pain with fever should not be brushed off.
Returning To Heavy Meals Too Fast
After feeling better, it is tempting to jump back into greasy, oversized, or very heavy meals. A gradual return is usually easier on the digestive system.
Avoiding Fiber Forever
A temporary low-fiber phase during recovery is not the same as a permanent low-fiber lifestyle. Long-term prevention often points in the opposite direction.
Becoming Overly Restrictive
Some people end up eating almost nothing out of fear. That can create new problems such as poor nutrition, low energy, and unnecessary anxiety.
Conclusion
Acute diverticulitis is an inflammatory condition of the colon that can range from uncomfortable to serious. The hallmark symptom is usually steady lower abdominal pain, often on the left side, especially when it is paired with tenderness, fever, nausea, or changes in bowel habits.
The most important practical takeaway is this: location, persistence, and severity matter. A painful belly that keeps getting worse is not something to guess at. Proper evaluation can help confirm the diagnosis, rule out look-alike conditions, and determine whether the episode is uncomplicated or complicated.
Recovery often includes a short-term diet adjustment, hydration, rest, and careful follow-up. Long-term prevention usually centers on consistent habits rather than quick fixes: more fiber after recovery, regular movement, good hydration, weight management, smoking avoidance, and attention to bowel habits.
If you have had an episode of acute diverticulitis, your next best step is not panic. It is a clear plan. Know your symptoms, understand your recovery stage, follow medical advice, and build the daily habits that support colon health over time.